
Abstract
Protein ingestion following resistance-type exercise stimulates muscle protein synthesis rates and consequently enhances the skeletal muscle adaptive response to prolonged training. Ingestion of ~ 20 g of quickly digestible protein isolate optimizes muscle protein synthesis rates during the first few hours of post-exercise recovery. However, the majority of daily protein intake is consumed as slower digestible, nutrient-rich, whole-food protein sources as part of mixed meals. Therefore, the muscle protein synthetic response to the ingestion of protein supplements and typical foods or mixed meals may differ substantially. In addition, the muscle protein synthetic response to feeding is not only determined by acute nutrient intake but is also likely modulated by habitual energy and nutrient intake and nondietary factors such as habitual physical activity, body composition, age, and/or sex. Therefore, nutritional recommendations to maximize the muscle protein synthetic response to exercise depend on the type of meal (e.g., protein supplements vs. mixed meals) and the time until the next feeding opportunity (e.g., feeding before overnight sleep) and, therefore, need to be personalized to the individual athlete.
Similar content being viewed by others


Ingestion of 20 g of isolated, quickly digestible protein results in a near-maximal muscle protein synthetic response at rest and post-exercise, with a 10–20% further increase when the ingested amount is doubled to 40 g. |
The ingestion of ≥ 40 g of slow digestible protein is recommended to maximize muscle protein synthesis rates when there is a prolonged period until the next feeding opportunity (≥ 6 h, e.g., overnight sleep). |
Nutritional recommendations to optimize the muscle protein synthetic response to feeding should be personalized to the individual athlete (i.e., age, sex, and body composition, and type, intensity, and duration of exercise). |
1 Introduction
While muscle mass is remarkably constant in healthy adults, it is a highly adaptive organ capable of changing in size and/or function. Even when muscle mass is constant, muscle tissue is constantly turning over, i.e., the rates at which muscle proteins are synthesized and broken down are in balance. This turnover allows muscle tissue to remodel, e.g., replacing damaged proteins with new proteins or changing the composition of muscle proteins to adapt to challenges such as exercise. An imbalance between protein synthesis and protein breakdown rates in skeletal muscle results in either a net gain (synthesis > breakdown) or net loss (breakdown > synthesis) in muscle mass.
A single session of exercise stimulates muscle protein synthesis (MPS) rates and, to a lesser extent, muscle protein breakdown rates [1, 2]. However, muscle protein net balance will remain negative in the absence of food intake [2]. Protein ingestion stimulates MPS and inhibits muscle protein breakdown rates, resulting in net muscle protein accretion during the acute stages of post-exercise recovery [3]. Therefore, post-exercise protein ingestion is widely applied as a strategy to augment post-exercise MPS rates and, as such, to facilitate the skeletal muscle adaptive response to prolonged exercise training.
Various factors have been identified that can modulate the MPS response to feeding, including the amount [4, 5], type [6, 7], and timing [8] of protein ingestion. However, much of this work has focused on isolated amino acids or quickly digestible protein isolates ingested in the absence of other nutrients [4,5,6, 8]. Such conditions may not be reflective of the postprandial MPS response to the ingestion of a mixed meal, in which protein is typically consumed in the form of slower digestible, whole-food protein sources [9]. In addition, the MPS response to feeding is not only determined by acute nutrient intake (i.e., meal composition) but is also likely modulated by habitual energy and nutrient intake and nondietary factors such as habitual physical activity, body composition, age, and/or sex [2, 10,11,12,13]. Therefore, nutritional recommendations to maximize the MPS response to feeding may depend on the type of meal (e.g., protein supplements vs. mixed meals) and time until the next feeding opportunity (e.g., feeding before overnight sleep) and should be personalized to the individual (e.g., accounting for physical activity level). While protein ingestion has been shown to stimulate the post-exercise MPS response following various modes of exercise [14,15,16], the majority of work has focused on resistance-type exercise. Therefore, the purpose of this review is to discuss our current understanding of dietary and nondietary factors modulating the MPS response to feeding and following resistance-type exercise.
2 Acute Dietary Factors Modulating the Muscle Protein Synthetic Response to Feeding
2.1 Amount of Protein
Few studies have investigated the dose–response relationship between protein ingestion and MPS rates during recovery from resistance-type exercise in younger adults. Moore et al. [4] were the first to present a dose response in MPS rates following the ingestion of 0, 5, 10, 20, or 40 g of egg protein during recovery from lower-body exercise. They observed a dose-dependent increase in MPS rates up to the ingestion of 20 g of protein, with a nonsignificant ~ 10% further increase following the ingestion of 40 g (Fig. 1a). Witard et al. [5] followed up on this work by assessing the impact of ingesting increasing amounts of whey protein on MPS rates at rest and during post-exercise recovery using a unilateral leg exercise model. In addition, subjects ingested a standardized protein-rich breakfast 4 h before ingestion of the protein beverages. The ingestion of 20 g of whey protein was sufficient to maximize MPS rates at rest and during post-exercise recovery, with a nonsignificant ~ 10% further increase following the ingestion of 40 g of protein in the post-exercise condition. More recently, the ingestion of 20 g and 40 g of whey protein were compared in a crossover design following whole-body resistance-type exercise [17]. The 40 g dose resulted in significant 20% higher MPS rates compared with the 20 g dose. These data may suggest that the amount of protein required to maximize MPS rates following whole-body resistance-type exercise is higher when compared with exercise during which less muscle is recruited. However, this hypothesis requires confirmation in a more direct comparison. Taken together, it appears that the ingestion of 20 g of isolated, quickly digestible protein results in a near-maximal MPS response at rest and post-exercise, with a 10–20% further increase when the ingested amount is doubled to 40 g (Fig. 1a).

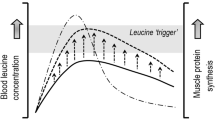
Conceptual representation of the muscle protein synthesis (MPS) response to various feeding protocols. a The ingestion of ~ 20 g quickly digestible protein results in a near-maximal MPS response. b The ingestion of 20 g plant-based protein typically results in a submaximal MPS response, but the consumption of a greater amount and/or mixing different sources may possibly augment the MPS response. c The ingestion of 20 g slowly digestible protein results in a submaximal MPS response, but the ingestion of greater amounts may result in a more prolonged anabolic response. d Mixed meal ingestion may result in a more moderate but prolonged MPS response compared with ingestion of an isolated whole-food protein source. The micronutrient content of a whole-food protein source may further augment the MPS response. iAUC incremental area under the curve
The impact of varying amounts of ingested protein on post-exercise MPS rates in young adults has been limited to experimental settings investigating the impact of ingesting isolated, quickly digestible protein sources on MPS rates during 4–5 h of post-exercise recovery [4, 5, 17]. These conditions are ecologically valid for the acute post-exercise period in which the ingestion of quickly digestible protein supplements is common practice. However, such conditions do not reflect most meal situations in which protein is generally consumed as slower digestible, nutrient-rich, whole-food protein sources as part of a mixed meal. Therefore, it should be questioned whether these data can be directly translated to per-meal protein recommendations.
2.2 Type of Protein
Plant-based protein sources are typically considered less efficient at stimulating MPS rates than animal-based protein sources. The possible lower anabolic properties of plant-based protein sources may be attributed to the lower total essential amino acid content, limited content of specific amino acids, lower leucine content, lower digestibility, and/or higher splanchnic extraction of plant-based protein-derived amino acids [18]. Indeed, most studies show that the ingestion of animal-based protein sources generally results in higher MPS rates at rest or following resistance-type exercise than plant-based protein sources in younger and older adults [6, 7, 19]. We have recently observed a significant increase in MPS in older adults following the ingestion of 60 g of wheat protein hydrolysate but not following the ingestion of 35 g of wheat protein hydrolysate [19]. These data suggest that consumption of a greater amount of plant-based protein is an effective strategy to compensate for its lower quality. However, whether the ingestion of large amounts of plant-based protein can maximize MPS rates in younger adults and/or following resistance-type exercise remains to be determined (Fig. 1b). It is important to note that investigations of the impact of plant-based protein sources on MPS rates has been limited to the ingestion of protein isolates. A typical mixed meal is likely to also include some animal-based protein and/or contain different plant-based protein sources that may provide a more balanced amino acid profile [20]. Therefore, the proposed lower MPS response to the ingestion of a single plant-based protein source can potentially be rescued by the ingestion of multiple (plant-based) protein sources (Fig. 1b).
2.3 Protein Digestion and Absorption Rate
Dietary protein sources can differ substantially in their digestion and absorption kinetics. For example, whey is a quickly digestible protein that results in a rapid but transient postprandial increase in plasma amino acid concentrations [21]. In contrast, casein is a slower digestible protein that results in a more moderate but prolonged postprandial increase in plasma amino acid concentrations. The ingestion of whey protein typically stimulates MPS rates to a greater extent than casein protein when assessed over periods of up to 6 h at rest or following resistance-type exercise [6, 21, 22]. This has been attributed to the more rapid protein digestion and amino acid absorption kinetics as well as the higher leucine content in whey compared with casein protein, resulting in a more rapid rise in postprandial leucine concentrations [21, 23,24,25]. Furthermore, the post-exercise MPS response to whey protein ingestion is attenuated when ingested in multiple smaller doses over time versus bolus ingestion [26]. These data suggest that protein digestion and absorption kinetics, and timing of intake, modulate the MPS response even when amino acid composition is matched. Therefore, whether the optimal amount of ingested protein as established for quickly digestible protein sources can be translated to slower digestible protein sources can be questioned.
The post-exercise MPS response to the ingestion of different amounts of slow digestible protein has not been assessed in healthy young men. This response may have a temporal pattern that differs from that of more rapidly digested proteins. Increasing amounts of a more slowly digestible protein may result in a moderate but more prolonged MPS response consistent with its protein digestion and absorption pattern (Fig. 1c). Some support for this concept comes from our observations that the ingestion of 30 g of casein protein before sleep did not result in a detectable increase in overnight post-exercise MPS assessed over a prolonged 7.5-h overnight period [27], whereas we observed a ~ 22% increase in overnight MPS rates following the ingestion of 40 g of casein protein under nearly identical conditions [28]. While it should be noted that these studies assessed post-exercise MPS rates in different muscle protein fractions (i.e., mixed-muscle vs. myofibrillar protein), the ingestion of 30 g of protein should be more than sufficient to stimulate post-exercise mixed-muscle or myofibrillar protein synthesis rates over a 4–5 h period [4, 5]. Therefore, it appears that larger amounts of slow digestible protein are required to obtain a more robust stimulation of post-exercise MPS rates over more prolonged periods such as overnight sleep [29]. This may suggest that the optimal amount and type of ingested protein depends on the meal timing, with ~ 20 g of quickly digestible protein being preferred when there is a relatively short 3- to 5-h period until the next meal, but ingestion of ≥ 40 g of slower digestible protein may be favored when the period until the next feeding opportunity is prolonged. However, whether the digestion and absorption rate of a protein, and/or the co-ingestion of other nutrients, modulates the MPS response when relatively large amounts (≥ 40 g) of protein are ingested and MPS is assessed over a prolonged (> 6 h) period remains to be determined.
2.4 Mixed Meal Composition
Most work assessing the MPS response to feeding has focused on isolated protein intake. However, dietary protein is typically consumed as part of a mixed meal. The co-ingestion of foods that are not necessarily high in protein may still impact the total protein intake, the amino acid profile of the meal, protein digestion and absorption kinetics, hormonal response, and micronutrient intake. Such factors can potentially modulate the MPS response to feeding, but their individual contributions are difficult to predict [30].
Carbohydrate co-ingestion with protein delays protein absorption and digestion kinetics [31], although this does not seem to attenuate the MPS response to protein ingestion at rest or following resistance-type exercise [31, 32]. However, the impact of carbohydrate co-ingestion has been limited to the addition of rapidly digestible, high glycemic index carbohydrates to protein-containing beverages. In contrast, mixed meals are typically in solid form and provide more slowly digestible carbohydrates and also contain dietary fiber. Therefore, a greater delay in protein digestion and absorption kinetics can be expected following mixed meal ingestion compared with the ingestion of a protein–carbohydrate supplement. In support, the postprandial rise in plasma amino acid levels appears to be substantially attenuated when minced meat is consumed in a mixed meal [33, 34]. It has been suggested that carbohydrate co-ingestion may augment MPS rates via its ability to elicit a postprandial rise in insulin concentration. However, insulin is permissive for MPS during hyperaminoacidemia and does not stimulate MPS rates under conditions reflecting food ingestion at rest [35, 36]. Consistent with this notion, carbohydrate co-ingestion with protein does not augment MPS rates following resistance-type exercise [32].
Very little work has addressed the potential impact of fat co-ingestion on the MPS response to protein ingestion. Post-exercise amino acid uptake by the leg (indicative of muscle protein accretion) has been shown to be higher following the ingestion of high-fat milk compared with skim milk [37]. More recently, we observed no delay in protein digestion and amino acid absorption and the subsequent MPS rates when milk fat was co-ingested with a beverage containing casein protein in older adults at rest [38]. This absence of a delay in protein digestion and absorption kinetics may be attributed to layering of fat on top of protein in the stomach that may only occur with a liquid meal [39]. However, co-ingestion of 17 g of fat as provided by the consumption of whole eggs did not attenuate post-exercise protein digestion and absorption kinetics compared with the ingestion of an isonitrogenous amount of egg whites [40]. Therefore, fat co-ingestion does not appear to substantially impact protein digestion and amino acid absorption kinetics. However, there is some indication that an oversupply of lipid may impair postprandial MPS. We have shown that lipid infusion reduces the MPS response to the ingestion of amino acids during hyperinsulinemic-euglycemic clamped conditions in healthy younger adults at rest [41]. In addition, attenuated post-exercise intramuscular anabolic signaling (i.e., 4E-BP1 phosphorylation) has been observed following the combined ingestion of protein and fat compared with the combined ingestion of protein and carbohydrate [42]. The impact of the fat content of a protein-containing meal on the MPS response remains ambiguous.
Recent work suggests that the MPS response to feeding may be modulated by the consumption of micronutrients (Fig. 1d). In support, the ingestion of whole eggs was more effective in stimulating post-exercise MPS rates than was the ingestion of an isonitrogenous amount of egg whites [40]. The differential response could not be attributed to differences in protein digestion and amino acid absorption or caloric intake between the treatments [31, 32, 38]. A possible explanation is the considerably higher content of fat and/or micronutrients in whole eggs. As previously discussed, fat co-ingestion may augment the post-exercise MPS response to protein ingestion [37]. Furthermore, several micronutrients that are contained primarily in the yolk, such as vitamin A, vitamin D, vitamin E, zinc, selenium, and cholesterol, are potential candidates to augment the anabolic response to feeding [30, 43]. In addition, the co-ingestion of an amylopectin/chromium complex has recently been shown to augment the post-exercise MPS response to a suboptimal amount of protein [44]. However, it should be noted that some nutrients may potentially impair MPS when ingested in high amounts that are typically not found in whole foods. For example, the ingestion of the lipid second messenger phosphatidic acid has recently been shown to impair the post-exercise MPS response in older adults [45]. Furthermore, high-dose antioxidant supplementation (i.e., vitamin C and E) may blunt the adaptive response to exercise [46]. Therefore, high doses of micronutrient supplements with strong antioxidant properties is not recommended for athletes. Taken together, emerging evidence suggests that certain micronutrients in a meal may be able to modulate postprandial MPS rates. The MPS response to mixed meal ingestion may, therefore, differ from the ingestion of protein isolates due to changes in protein and amino acid absorption kinetics and/or specific micronutrient(s) content(s) (Fig. 1d).
To date, only one study has assessed postprandial MPS rates following mixed meal ingestion. Subjects consumed a ~ 1300 kcal lean beef mixed meal containing either 40 g or 70 g of protein [34]. Postprandial MPS rates did not differ between the ingestion of the moderate- or the high-protein meal at rest or during post-exercise recovery. Interestingly, plasma essential amino acid concentrations were highest at the end of the 4-h postprandial period. This may suggest that large protein-rich mixed meals result in a protein digestion and absorption pattern that reflects a more slowly digestible protein. Clearly, more research is warranted to assess the MPS response to the ingestion of mixed meals and its modulation by meal composition.
2.5 Alcohol
Despite warnings from health agencies, alcohol consumption remains culturally engrained worldwide [47]. Interestingly, several studies have reported that athletes are more likely to consume excessive amounts of alcohol, especially as part of binge-drinking practices in team sports [48, 49]. Parr et al. [15] demonstrated that alcohol ingestion impaired the MPS response to post-exercise protein ingestion. A total of 1.5 g alcohol per kg bodyweight (12 ± 2 standard drinks) was consumed to reflect alcohol intake levels reported in binge drinking practices of team athletes. These data provide clear proof of principle that ingestion of excessive amounts of alcohol can impair post-exercise recovery. Furthermore, Parr et al. [15] observed that alcohol co-ingestion downregulated intramuscular anabolic signaling (i.e., phosphorylation of mammalian target of rapamycin), which is consistent with the majority of data in rodent models [50]. How this alcohol-induced attenuation of anabolic signaling is regulated is unclear, but direct effects via REDD (regulated in development and DNA damage)-1 and indirect effects via the modulation of the activity of circulating anabolic hormones such as insulin-like growth factor 1 have been proposed [50]. Further work is required to provide more mechanistic insight and to determine whether there is a dose–response relationship between alcohol intake and MPS rates and to determine the impact of more moderate alcohol consumption, e.g., drinking one to two glasses of wine with dinner.
3 Habitual Food Intake and Postprandial Muscle Protein Synthesis
3.1 Habitual Energy and Protein Intake
The MPS response to feeding is not only modulated by acute nutrient intake but may also be affected by habitual food intake (Fig. 2). Athletes may intentionally eat a caloric surplus to gain lean body mass (i.e., bulking), but the impact of caloric overfeeding on MPS rates remains to be determined. It is more common for athletes to purposely restrict caloric intake to reduce body fat [51]. While it is feasible to increase lean body mass during a marked energy deficit when a high protein consumption is combined with a high volume of resistance and anaerobic exercise [52], energy restriction generally leads to muscle mass loss [53, 54]. Consistent with this notion, integrated MPS rates are reduced during energy restriction but can be rescued by resistance-type exercise and may be potentiated by a higher protein diet [55]. While acute caloric intake does not seem to modulate the MPS response to feeding [31, 38], both acute postabsorptive and postprandial MPS rates at rest have been shown to be attenuated following a short-term (3–14 day) energy intake restriction [10, 56]. Greater reductions in the MPS response to feeding can be expected during more severe energy deficits and in individuals with lower body fat levels, as these conditions have been shown to increase lean body mass loss during energy intake restriction [57, 58]. The blunted MPS response to protein ingestion during energy restriction may be rescued by the consumption of a higher protein diet. Subjects consuming 1.6 or 2.4 g protein/kg/day during a 40% energy deficit for 21 days had a preserved MPS response to protein ingestion, whereas this anabolic response was attenuated in subjects consuming the recommended daily allowance (RDA) for protein of 0.8 g/kg/day [59]. In contrast, the opposite pattern was observed in these subjects following 10 days of weight maintenance. A significant increase in MPS was observed in subjects ingesting 0.8 and 1.6 g of protein/kg/day, but no anabolic response was observed in subjects consuming 2.4 g of protein/kg/day [59]. We observed no impact of 14-day habituation to a higher (1.5 g/kg/day) or lower (0.7 g/kg/day) protein diet on postprandial MPS rates or the MPS response to the ingestion of 25 g of protein in weight-stable older adults. Furthermore, postabsorptive MPS rates do not appear to change even after a prolonged 12-week high (2.4 g/kg/day) or low (0.4 g/kg/day) protein diet in weight-stable healthy young adults [60]. While it is clear that prolonged energy restriction attenuates postabsorptive and postprandial MPS rates, the impact of habitual protein intake during energy restriction and energy balance on the MPS response to protein ingestion remains poorly understood.

Schematic representation of factors modulating the muscle protein synthetic (MPS) response to feeding. The MPS response to feeding is augmented by prior exercise and a higher amount, essential amino acid (EEA) content, and digestion and absorption rate of the ingested protein. The MPS response to feeding is attenuated by alcohol co-ingestion, during prolonged energy deficit, during muscle inactivity, with aging (especially in females), and by individuals with excessive fat mass. ↑ indicates the MPS response to feeding is augmented, ↓ indicates the MPS response to feeding is attenuated, ↔ indicates the MPS response to feeding is not affected, ? indicates the impact on MPS response to feeding is unclear
3.2 Habitual Omega-3 Polyunsaturated Fatty Acid Intake
Omega-3 polyunsaturated fatty acid supplementation for 8 weeks has been shown to augment the MPS response to a hyperinsulinemic–hyperaminoacidic clamp in both younger and older adults [11, 61]. As postabsorptive MPS rates were not significantly increased following the supplementation period, omega-3 supplementation appears to specifically enhance the muscle anabolic sensitivity to hyperaminoacidemia. Insulin and amino acids were clamped to levels typically seen after a meal but were low enough to avoid a possible ceiling effect. In contrast, omega-3 supplementation for 8 weeks did not increase the MPS response to the ingestion of 30 g of whey protein at rest or following resistance-type exercise [62]. As 30 g of protein should be more than sufficient to maximize the MPS response to protein ingestion in healthy young subjects, it could be speculated that fish oil supplementation may only augment the MPS response to suboptimal amounts of protein ingestion. While omega-3 fatty acid supplementation could provide an effective nutritional strategy to augment the MPS response to protein ingestion, it is unclear what the target omega-3 concentrations should be and thus what dose and duration of supplementation period should be recommended.
4 Nondietary Factors Modulating the Muscle Protein Synthetic Response to Feeding
4.1 Exercise and Physical Activity
Physical activity and exercise are potent stimulators of postabsorptive as well as postprandial MPS rates [2, 63,64,65] (Fig. 2). A single bout of exercise stimulates the use of dietary protein-derived amino acids as precursors for MPS, as dietary protein-derived amino acids are more directed towards activated muscle during their recovery from exercise [66]. The MPS response to protein ingestion is maximally stimulated by the ingestion of 20 g of whey protein in rested conditions and following lower-body resistance-type exercise [4, 5], albeit with higher MPS rates during the post-exercise condition [4, 5]. However, exercise may increase not only the maximal rate of postprandial MPS but also the duration of the anabolic response. It has been suggested that the MPS response to protein ingestion is transient even in the presence of prolonged hyperaminoacidemia, a phenomenon often termed the “muscle full” effect [67]. However, the exercise-induced increase in anabolic sensitivity may supplant the muscle full effect and allow for a more prolonged MPS response to feeding. In support, two studies using a unilateral leg exercise model observed a prolonged MPS response to feeding in the exercised leg [68, 69]. MPS rates were elevated in the first 3 h following protein ingestion but had returned to basal levels in the subsequent 2 h in the rested leg, whereas MPS rates remained elevated during the entire 5-h period following protein ingestion in the exercised leg [68, 69]. Thus, exercise appears to increase both the rate and the duration of postprandial MPS rates.
MPS rates are also sensitive to habitual physical activity. Several studies have demonstrated that muscle disuse reduces postabsorptive and postprandial MPS rates following prolonged bed rest or immobilization [70,71,72,73]. Glover et al. [70] observed lower MPS rates during low- and high-dose amino acid infusion following 14 d of immobilization. As the higher amino acid infusion protocol provided ample amino acids to maximize the MPS response under normal conditions, it appears that hyperaminoacidemia cannot compensate for a disuse-induced decline in muscle anabolic sensitivity. Less extreme reductions in physical activity may also reduce anabolic sensitivity in muscle. For example, a reduction in daily step count has also been shown to reduce the MPS response to feeding in older adults [72]. To date, the impact of step reduction on MPS rates in healthy younger adults has not been assessed. It could be speculated that a reduction in daily step count has less impact on anabolic sensitivity in athletes undergoing intensive exercise training, as low-load resistance-type exercise has been shown to attenuate the decline in anabolic sensitivity during step reduction in older adults [71]. However, the MPS response to feeding is likely reduced during prolonged bed rest or immobilization and may contribute to injury-related muscle atrophy in athletes [74]. An injured athlete is likely to have a lower exercised-induced energy expenditure and is likely to reduce caloric intake to avoid gaining body fat. However, a reduction in energy intake may result in a lower absolute protein intake. While the limited work available does not support the idea that a higher protein intake can compensate for a disuse-induced reduction in MPS, habitual protein should at least be maintained [74, 75].
4.2 Ageing
Ageing is accompanied by a progressive decline in muscle mass, termed sarcopenia. Little to no differences in postabsorptive MPS rates are observed between younger and older adults [76, 77]. However, the MPS response to feeding is attenuated in older compared with younger adults, a phenomenon termed anabolic resistance [77]. Interestingly, it appears the age-related anabolic resistance to protein ingestion can be at least partly compensated for by increasing the amount of ingested protein. Whereas the ingestion of 20 g of high-quality protein appears sufficient to maximize the MPS response at rest or during post-exercise recovery in younger adults [4, 5], no clear plateau in postprandial MPS rates following graded doses up to ~ 40 g of ingested whey, beef, or soy protein has been observed in older adults at rest or during post-exercise recovery [78]. Therefore, possibly even greater amounts of ingested protein are required to maximize the MPS response to feeding in older adults. Alternatively, it is not clear whether 40 g of dietary protein is required to maximize the anabolic response in older adults or whether a more moderate dose such as 30 g is sufficient. Some support for the latter comes from a retrospective biphase linear regression and breakpoint analysis that observed a dose–response relation between protein ingestion and postprandial MPS rates up to ~ 0.4 g/kg bodyweight in older adults at rest [79]. The average weight of the older adults in this analysis was 79.3 kg, which would suggest that the average older adult of ~ 80 kg would require ~ 30 g of protein in a meal to maximize the MPS response at rest. Therefore, older athletes should aim to ingest at least 30 g of high-quality protein per meal to improve exercise recovery and adaptations.
4.3 Sex
Men have more muscle mass and less body fat than age- and bodyweight-matched females [80]. However, in healthy young adults, no such sexual dimorphism is apparent in basal MPS rates [11, 81,82,83], MPS response to a hyperinsulinemic–hyperaminoacidemic clamp [11, 83], MPS response to resistance-type exercise [82], or postprandial MPS rates following resistance-type exercise [81]. A possible explanation for this apparent discrepancy is that the greater amount of muscle mass in males than in females primarily originates from an augmented growth spurt in males during puberty, which seems attributable to the surge in testosterone secretion [13, 84]. After puberty, muscle mass remains largely constant up to middle-age adulthood in both healthy males and healthy females, which is consistent with similar muscle protein turnover rates between the sexes. Therefore, nutritional strategies to maximize the muscle anabolic response do not differ between young male and female adults per se.
In contrast to younger adults, a sexual dimorphism in MPS rates may exist in adults at a more advanced age. Older women have higher postabsorptive MPS rates but a blunted MPS response to feeding compared with older men at rest [13, 83, 85]. As greater amounts of protein in a meal can at least partly compensate for age-related anabolic resistance [78], it is tempting to speculate that older women require the ingestion of higher amounts of protein to maximize the anabolic response to feeding when compared with older men. In addition, whether age-related sexual dimorphism in the MPS response to protein feeding is present in active older adults engaging in regular exercise training remains to be determined.
4.4 Body Size
It seems intuitive that individuals with a greater lean body mass require larger amounts of protein to be consumed than do individuals with less lean body mass. Consistent with this line of thinking, protein intake requirements are often expressed relative to body size, and most typically to body weight, as this is more practical to assess in individuals. However, only one study has directly examined the impact of body size on the MPS response to feeding. Macnaughton et al. [17] observed no difference in the post-exercise MPS response to protein ingestion between subjects with a relatively small or large amount of fat free mass (~ 59 vs. 77 kg, respectively). These data suggest that lean body mass is not a strong modulator of protein requirements in the initial several hours of post-exercise recovery. A possible explanation is that only a relatively small amount of essential amino acids is required as precursors for MPS, even in larger individuals. A factor that is more likely to limit the MPS response to feeding is the postprandial rise in plasma leucine concentration [68]. However, Macnaughton et al. [17] observed only a trivial difference in peak plasma leucine levels following protein ingestion between smaller and larger individuals. Therefore, the amount of ingested protein required to maximize the muscle anabolic response following resistance-type exercise may be less affected by body size than has been assumed.
It is not uncommon for athletes in various sports such as rugby or bodybuilding to intentionally overfeed and gain considerable amounts of body fat in an attempt to optimize lean body mass gains (“bulking up”). However, several studies have reported attenuated postabsorptive and/or postprandial MPS rates in overweight or obese subjects at rest [12, 86,87,88], but these observations have not been consistent [12, 86,87,88,89]. What may cause a reduced MPS response to feeding in subjects with excess body fat is unclear, but it seems unlikely that the amount of body fat an individual possesses has a substantial impact on the amount of precursors required for MPS or the size of the plasma amino acid pool and consequently the peak plasma leucine concentrations following feeding. Therefore, it is more likely that excess body fat directly reduces anabolic sensitivity to protein ingestion in muscle. In support, lipid infusion has been shown to reduce postprandial MPS rates in healthy young adults at rest [41]. These data suggest that excess lipid availability per se reduces anabolic sensitivity within skeletal muscle, independent of body composition [41]. Therefore, athletes who are intentionally overfeeding to gain muscle mass may consider limiting excessive dietary fat intake and body fat accumulation. However, the proposed impact of excessive body fat mass on MPS rates is likely confounded by habitual physical activity levels and is perhaps less of a concern for athletes engaged in regular intense exercise training.
5 Is the Anabolic Response to Feeding Limited to Muscle Protein Synthesis?
5.1 Muscle Protein Breakdown
It could be argued that the anabolic response to feeding is not limited to the MPS response. Muscle protein net balance is determined by the difference between MPS and muscle protein breakdown rates. However, changes in MPS rates in response to exercise and nutrition seem to be much greater than changes observed in muscle protein breakdown rates [2, 90]. Therefore, changes in net muscle protein balance appear to be largely determined by changes in MPS rates. While feeding reduces muscle protein breakdown rate via an increase in circulating plasma insulin concentrations, only a moderate rise in insulin concentration is required for maximal inhibition of muscle breakdown rates. Greenhaff et al. [35] assessed the impact of a constant amino acid infusion together with progressive increments in insulin on muscle protein breakdown rates and found that increasing insulin concentrations to 30 mU/L lowered muscle protein breakdown rates by ~ 50% compared with basal levels, with no further suppression at higher insulin concentrations. However, it appears even lower insulin concentrations may be sufficient to suppress post-exercise muscle protein breakdown rates. The ingestion of 20–25 g of protein increases insulin concentrations to ~ 15–20 mU/L, with no further suppression in post-exercise muscle protein breakdown rates when insulin levels are increased to ~ 65 mU/L via carbohydrate co-ingestion [32]. Therefore, food intake will substantially reduce muscle protein breakdown rates, with the macronutrient content of the food being of little impact.
Although under normal, healthy conditions, protein breakdown does not seem to play an important quantitative role in net muscle accretion, it does have an important function in muscle tissue reconditioning. Proteolysis is required for the clearance of damaged and/or aberrant proteins, thereby allowing optimal tissue function and remodeling. In support, knocking out critical genes in the protein breakdown proteasome and autophagy pathways reduces muscle quality, muscle function, and muscle mass in animal models [91,92,93,94]. These data suggest that at least some amount of muscle protein breakdown is required for proper muscle conditioning. Therefore, inhibition of muscle protein breakdown beyond the normal postprandial reduction may not represent a desirable target in healthy populations.
5.2 Whole-Body Protein Balance
Assessment of MPS and/or breakdown rates requires sampling of skeletal muscle tissue. To avoid skeletal muscle tissue sampling, protein synthesis and protein breakdown rates are often assessed on a whole-body level, which only requires stable isotope tracer infusion and arterial or arterialized blood sampling [95]. As muscle tissue represents a large proportion (~ 40%) of total body protein content, it is often assumed that whole-body protein metabolism is a good proxy for muscle tissue protein turnover. However, muscle tissue has a relatively slow turnover when compared with other tissues, such as liver, kidney, lung, intestine [96], and even brain [97]. Therefore, muscle mass is estimated to contribute only ~ 25–30% to whole-body protein turnover [98]. As a consequence, whole-body and MPS rates in response to nutrition [27, 34, 40], exercise [65, 99], and disease [100, 101] do not necessarily align. Although ample data are available on the impact of various stimuli on muscle tissue protein synthesis and/or breakdown rates, the responsiveness of other tissues to similar factors is less well studied. Consequently, we should be cautious when applying whole-body amino acid kinetics to gain insight into protein metabolism at a tissue-specific level.
Practical inferences based on the assessment of whole-body protein metabolism are further complicated by methodological issues. A common method to assess whole-body protein metabolism is based on the amino acid flux in and out of the circulation. This method assumes that the rate at which amino acids are disappearing from the circulation (i.e., tissue uptake) minus amino acid oxidation rates reflects whole-body protein synthesis. This would require the tissue free amino acid pools to remain constant. However, tissue free amino acid pools are likely to change considerably in response to conditions such as feeding, invalidating whole-body protein synthesis rate calculations. Even more complex is the determination of whole-body protein breakdown rates in a postprandial setting. Whole-body protein breakdown rates are determined by the rate at which amino acids are appearing in the circulation from tissues minus the rate at which dietary protein-derived amino acids appear in the circulation. Therefore, calculation of whole-body protein breakdown rates depends on accurate assessment of the amount of exogenous protein appearing in the circulation. Some researchers estimate the latter based on previously published values [34, 102, 103]. However, such values are specific to the experimental conditions under which they are obtained (i.e., the amount and type of protein, the pattern of protein ingestion, and the duration of the postprandial period assessed), and may not be applicable to other conditions. Therefore, assessment of postprandial whole-body protein breakdown rates is only reliable when the amount of exogenous protein appearing in the circulation is assessed appropriately [104].
The indicator amino acid technique is a noninvasive method to assess whole-body protein balance [105]. The ingestion of ~ 50 g of protein maximizes whole-body protein balance in healthy adult males following intermittent-type exercise as assessed by the indicator amino acid technique [106]. In contrast, the ingestion of 20–40 g of high-quality protein is sufficient to maximize the postprandial MPS response in healthy young adults at rest or following resistance-type exercise [4, 5, 17]. Therefore, athletes determined to maximize anabolism in both muscle and non-muscle tissues may consider the ingestion of ~ 50 g of protein per meal. However, clearly more research is warranted to determine which non-muscle tissues are responsive to protein feeding and whether this has any functional relevance for athletes.
5.3 Do Myofibrillar Protein Synthesis Rates Reflect Changes in Muscle Mass?
Whether changes in MPS rates following certain stimuli correlate with subsequent changes in muscle mass during more prolonged exposure to such stimuli has been questioned. Mitchell et al. [107] observed no correlations between acute post-exercise myofibrillar protein synthesis rates and muscle hypertrophy observed following more prolonged resistance-type exercise training. Myofibrillar protein synthesis rates were assessed in the first 6 h following the first exercise bout performed as part of the prolonged exercise training program. The lack of significant (positive) correlations is not surprising as basal and postprandial myofibrillar protein synthesis rates have been shown to be elevated for up to 72 h after a single bout of exercise [63]. A follow-up study assessed myofibrillar protein synthesis rates during a more prolonged 48-h post-exercise period after the initial exercise bout, at 3 weeks, and at 10 weeks of a prolonged resistance-type exercise training program [108]. While no correlations were observed between post-exercise myofibrillar protein synthesis rates following the initial exercise bout and muscle hypertrophy following prolonged exercise training, strong positive correlations were observed between myofibrillar protein synthesis rates assessed over a 48-h period at 3 weeks and at 10 weeks of training and the increase in muscle mass. The initial exercise bout resulted in considerable muscle damage, but exercise-induced muscle damage was attenuated at 3 weeks of training and almost completely absent at 10 weeks. Therefore, it appears that the myofibrillar protein synthetic response to a single bout of unaccustomed exercise may be at least partly a response to muscle damage and directed at tissue repair rather than muscle hypertrophy. After the first couple of days or weeks of training, post-exercise myofibrillar protein synthesis rates may be more reflective of the net changes in muscle mass, i.e., muscle hypertrophy. Consistent with this notion, myofibrillar protein synthesis rates assessed during several weeks of a prolonged resistance-type training program have been shown to correlate with muscle hypertrophy [109]. Given these findings, it seems evident that changes in myofibrillar protein synthesis rates during recovery from successive exercise sessions can be predictive of net increase in muscle mass.
6 Conclusions
The ingestion of 20 g of high-quality, rapidly digestible protein results in a near-maximal stimulation of MPS rates at rest and during the initial several hours of recovery following lower-body resistance-type exercise. Ingestion of animal-derived proteins tends to result in a greater increase in MPS rates than ingestion of plant-derived proteins. However, ingestion of larger amounts and/or mixing of different plant-derived proteins may possibly compensate for the lower anabolic properties. The ingestion of relatively large amounts (≥ 40 g) of slowly digestible protein may result in a prolonged MPS response and may be recommendable when there is a prolonged period until the next feeding opportunity (≥ 6 h, e.g., overnight sleep). Recent evidence suggests that whole-food protein sources may contain micronutrients that can further augment the MPS response. The anabolic response to protein ingestion is attenuated during prolonged energy intake restriction, during muscle disuse, and in older adults (especially older females). The ingestion of greater amounts of protein can at least partly rescue the blunted MPS response during prolonged energy restriction and ageing but not during muscle disuse. In conclusion, nutritional recommendations to maximize the MPS response to feeding depend on both the type of meal and time until the next feeding opportunity and should be personalized to the individual athlete.
References
Biolo G, Maggi SP, Williams BD, Tipton KD, Wolfe RR. Increased rates of muscle protein turnover and amino acid transport after resistance exercise in humans. Am J Physiol. 1995;268:E514–20.
Phillips SM, Tipton KD, Aarsland A, Wolf SE, Wolfe RR. Mixed muscle protein synthesis and breakdown after resistance exercise in humans. Am J Physiol. 1997;273:E99–107.
Tipton KD, Ferrando AA, Phillips SM, Doyle DJ, Wolfe RR. Postexercise net protein synthesis in human muscle from orally administered amino acids. Am J Physiol. 1999;276:E628–34.
Moore DR, Robinson MJ, Fry JL, Tang JE, Glover EI, Wilkinson SB, et al. Ingested protein dose response of muscle and albumin protein synthesis after resistance exercise in young men. Am J Clin Nutr. 2009;89:161–8.
Witard OC, Jackman SR, Breen L, Smith K, Selby A, Tipton KD. Myofibrillar muscle protein synthesis rates subsequent to a meal in response to increasing doses of whey protein at rest and after resistance exercise. Am J Clin Nutr. 2013;99:86–95.
Tang JE, Moore DR, Kujbida GW, Tarnopolsky MA, Phillips SM. Ingestion of whey hydrolysate, casein, or soy protein isolate: effects on mixed muscle protein synthesis at rest and following resistance exercise in young men. J Appl Physiol. 1985;2009(107):987–92.
Wilkinson SB, Tarnopolsky MA, Macdonald MJ, Macdonald JR, Armstrong D, Phillips SM. Consumption of fluid skim milk promotes greater muscle protein accretion after resistance exercise than does consumption of an isonitrogenous and isoenergetic soy-protein beverage. Am J Clin Nutr. 2007;85:1031–40.
Levenhagen DK, Gresham JD, Carlson MG, Maron DJ, Borel MJ, Flakoll PJ. Postexercise nutrient intake timing in humans is critical to recovery of leg glucose and protein homeostasis. Am J Physiol Endocrinol Metab. 2001;280:E982–93.
Gorissen SHM, Remond D, van Loon LJC. The muscle protein synthetic response to food ingestion. Meat Sci. 2015;109:96–100.
Hector AJ, Marcotte GR, Churchward-Venne TA, Murphy CH, Breen L, Von Allmen M, et al. Whey protein supplementation preserves postprandial myofibrillar protein synthesis during short-term energy restriction in overweight and obese adults. J Nutr. 2015;145:246–52.
Smith GI, Atherton P, Reeds DN, Mohammed BS, Rankin D, Rennie MJ, et al. Omega-3 polyunsaturated fatty acids augment the muscle protein anabolic response to hyperinsulinaemia–hyperaminoacidaemia in healthy young and middle-aged men and women. Clin Sci (Lond). 2011;121:267–78.
Beals JW, Sukiennik RA, Nallabelli J, Emmons RS, van Vliet S, Young JR, et al. Anabolic sensitivity of postprandial muscle protein synthesis to the ingestion of a protein-dense food is reduced in overweight and obese young adults. Am J Clin Nutr. 2016;104:1014–22.
Smith GI, Mittendorfer B. Sexual dimorphism in skeletal muscle protein turnover. J Appl Physiol. 1985;2016(120):674–82.
Moore DR, Camera DM, Areta JL, Hawley JA. Beyond muscle hypertrophy: why dietary protein is important for endurance athletes 1. Appl Physiol Nutr Metab. 2014;39:987–97.
Parr EB, Camera DM, Areta JL, Burke LM, Phillips SM, Hawley JA, et al. Alcohol ingestion impairs maximal post-exercise rates of myofibrillar protein synthesis following a single bout of concurrent training. PLoS One. 2014;9:e88384.
Pasiakos SM, McClung HL, Margolis LM, Murphy NE, Lin GG, Hydren JR, et al. Human muscle protein synthetic responses during weight-bearing and non-weight-bearing exercise: a comparative study of exercise modes and recovery nutrition. PLoS One. 2015;10:e0140863.
Macnaughton LS, Wardle SL, Witard OC, McGlory C, Hamilton DL, Jeromson S, et al. The response of muscle protein synthesis following whole-body resistance exercise is greater following 40 g than 20 g of ingested whey protein. Physiol Rep 2016;4(15). pii:e12893.
van Vliet S, Burd NA, van Loon LJ. The skeletal muscle anabolic response to plant- versus animal-based protein consumption. J Nutr. 2015;145:1981–91.
Gorissen SH, Horstman AM, Franssen R, Crombag JJ, Langer H, Bierau J, et al. Ingestion of wheat protein increases in vivo muscle protein synthesis rates in healthy older men in a randomized trial. J Nutr. 2016;146:1651–9.
Reidy PT, Walker DK, Dickinson JM, Gundermann DM, Drummond MJ, Timmerman KL, et al. Protein blend ingestion following resistance exercise promotes human muscle protein synthesis. J Nutr. 2013;143:410–6.
Pennings B, Boirie Y, Senden JMG, Gijsen AP, Kuipers H, van Loon LJC. Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older men. Am J Clin Nutr. 2011;93:997–1005.
Burd NA, Yang Y, Moore DR, Tang JE, Tarnopolsky MA, Phillips SM. Greater stimulation of myofibrillar protein synthesis with ingestion of whey protein isolate v. micellar casein at rest and after resistance exercise in elderly men. Br J Nutr. 2012;108:958–62.
Koopman R, Crombach N, Gijsen AP, Walrand S, Fauquant J, Kies AK, et al. Ingestion of a protein hydrolysate is accompanied by an accelerated in vivo digestion and absorption rate when compared with its intact protein. Am J Clin Nutr. 2009;90:106–15.
Wall BT, Hamer HM, de Lange A, Kiskini A, Groen BBL, Senden JMG, et al. Leucine co-ingestion improves post-prandial muscle protein accretion in elderly men. Clin Nutr. 2013;32:412–9.
Devries MC, Phillips SM. Supplemental protein in support of muscle mass and health: advantage whey. J Food Sci. 2015;80(Suppl 1):A8–15.
West DWD, Burd NA, Coffey VG, Baker SK, Burke LM, Hawley JA, et al. Rapid aminoacidemia enhances myofibrillar protein synthesis and anabolic intramuscular signaling responses after resistance exercise. Am J Clin Nutr. 2011;94:795–803.
Trommelen J, Kouw IWK, Holwerda AM, Snijders T, Halson SL, Rollo I, et al. Pre-sleep dietary protein-derived amino acids are incorporated in myofibrillar protein during post-exercise overnight recovery. Am J Physiol Endocrinol Metab. 2018;314:E457–67.
Res PT, Groen B, Pennings B, Beelen M, Wallis GA, Gijsen AP, et al. Protein ingestion before sleep improves postexercise overnight recovery. Med Sci Sports Exerc. 2012;44:1560–9.
Trommelen J, van Loon LJC. Pre-sleep protein ingestion to improve the skeletal muscle adaptive response to exercise training. Nutrients. 2016;8(12). pii:E763.
Vliet SV, Beals JW, Martinez IG, Skinner SK, Burd NA. Achieving optimal post-exercise muscle protein remodeling in physically active adults through whole food consumption. Nutrients. 2018;10:224.
Gorissen SHM, Burd NA, Hamer HM, Gijsen AP, Groen BB, van Loon LJC. Carbohydrate coingestion delays dietary protein digestion and absorption but does not modulate postprandial muscle protein accretion. J Clin Endocrinol Metab. 2014;99:2250–8.
Staples AW, Burd NA, West DWD, Currie KD, Atherton PJ, Moore DR, et al. Carbohydrate does not augment exercise-induced protein accretion versus protein alone. Med Sci Sports Exerc. 2011;43:1154–61.
Pennings B, Groen BBL, van Dijk J-W, de Lange A, Kiskini A, Kuklinski M, et al. Minced beef is more rapidly digested and absorbed than beef steak, resulting in greater postprandial protein retention in older men. Am J Clin Nutr. 2013;98:121–8.
Kim I-Y, Schutzler S, Schrader A, Spencer HJ, Azhar G, Ferrando AA, et al. The anabolic response to a meal containing different amounts of protein is not limited by the maximal stimulation of protein synthesis in healthy young adults. Am J Physiol Endocrinol Metab. 2016;310:E73–80.
Greenhaff PL, Karagounis LG, Peirce N, Simpson EJ, Hazell M, Layfield R, et al. Disassociation between the effects of amino acids and insulin on signaling, ubiquitin ligases, and protein turnover in human muscle. Am J Physiol Endocrinol Metab. 2008;295:E595–604.
Trommelen J, Groen BBL, Hamer HM, de Groot LCPGM, van Loon LJC. Mechanisms in endocrinology: exogenous insulin does not increase muscle protein synthesis rate when administered systemically: a systematic review. Eur J Endocrinol. 2015;173:R25–34.
Elliot TA, Cree MG, Sanford AP, Wolfe RR, Tipton KD. Milk ingestion stimulates net muscle protein synthesis following resistance exercise. Med Sci Sports Exerc. 2006;38:667–74.
Gorissen SHM, Burd NA, Kramer IF, van Kranenburg J, Gijsen AP, Rooyackers O, et al. Co-ingesting milk fat with micellar casein does not affect postprandial protein handling in healthy older men. Clin Nutr. 2015;36:429–37.
Edelbroek M, Horowitz M, Maddox A, Bellen J. Gastric emptying and intragastric distribution of oil in the presence of a liquid or a solid meal. J Nucl Med. 1992;33:1283–90.
van Vliet S, Shy EL, Abou Sawan S, Beals JW, West DW, Skinner SK, et al. Consumption of whole eggs promotes greater stimulation of postexercise muscle protein synthesis than consumption of isonitrogenous amounts of egg whites in young men. Am J Clin Nutr. 2017;106:1401–12.
Stephens FB, Chee C, Wall BT, Murton AJ, Shannon CE, van Loon LJC, et al. Lipid-induced insulin resistance is associated with an impaired skeletal muscle protein synthetic response to amino acid ingestion in healthy young men. Diabetes. 2015;64:1615–20.
Hammond KM, Impey SG, Currell K, Mitchell N, Shepherd SO, Jeromson S, et al. Postexercise high-fat feeding suppresses p70S6K1 activity in human skeletal muscle. Med Sci Sports Exerc. 2016;48:2108–17.
Riechman SE, Andrews RD, Maclean DA, Sheather S. Statins and dietary and serum cholesterol are associated with increased lean mass following resistance training. J Gerontol A Biol Sci Med Sci. 2007;62:1164–71.
Ziegenfuss TN, Lopez HL, Kedia A, Habowski SM, Sandrock JE, Raub B, et al. Effects of an amylopectin and chromium complex on the anabolic response to a suboptimal dose of whey protein. J Int Soc Sports Nutr. 2017;14:6.
Smeuninx B, Nishimura Y, Mckendry J, Limb M, Smith K, Atherton PJ, et al. The effect of acute oral phosphatidic acid ingestion on myofibrillar protein synthesis and intracellular signaling in older males. Clin Nutr. 2018;S0261–5614(18):31182–8.
Bjornsen T, Salvesen S, Berntsen S, Hetlelid KJ, Stea TH, Lohne-Seiler H, et al. Vitamin C and E supplementation blunts increases in total lean body mass in elderly men after strength training. Scand J Med Sci Sports. 2016;26:755–63.
World Health Organization. World Health Organization. Management of substance abuse unit. Global status report on alcohol and health, 2014. Geneva: World Health Organization; 2014.
Burke LM, Read RS. A study of dietary patterns of elite Australian football players. Can J Sport Sci. 1988;13:15–9.
Watten RG. Sports, physical exercise and use of alcohol. Scand J Med Sci Sports. 1995;5:364–8.
Steiner JL, Lang CH. Dysregulation of skeletal muscle protein metabolism by alcohol. Am J Physiol Endocrinol Metab. 2015;308:E699–712.
Sundgot-Borgen J, Garthe I. Elite athletes in aesthetic and Olympic weight-class sports and the challenge of body weight and body compositions. J Sports Sci. 2011;29(Suppl 1):S101–14.
Longland TM, Oikawa SY, Mitchell CJ, Devries MC, Phillips SM. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: a randomized trial. Am J Clin Nutr. 2016;103:738–46.
Weinheimer EM, Sands LP, Campbell WW. A systematic review of the separate and combined effects of energy restriction and exercise on fat-free mass in middle-aged and older adults: implications for sarcopenic obesity. Nutr Rev. 2010;68:375–88.
Backx EMP, Tieland M, van den Borgonjen Berg KJ, Claessen PR, van Loon LJC, de Groot LCPGM. Protein intake and lean body mass preservation during energy intake restriction in overweight older adults. Int J Obes (Lond). 2016;40:299–304.
Hector AJ, McGlory C, Damas F, Mazara N, Baker SK, Phillips SM. Pronounced energy restriction with elevated protein intake results in no change in proteolysis and reductions in skeletal muscle protein synthesis that are mitigated by resistance exercise. FASEB J. 2018;32:265–75.
Areta JL, Burke LM, Camera DM, West DWD, Crawshay S, Moore DR, et al. Reduced resting skeletal muscle protein synthesis is rescued by resistance exercise and protein ingestion following short-term energy deficit. Am J Physiol Endocrinol Metab. 2014;306:E989–97.
Garthe I, Raastad T, Refsnes PE, Koivisto A, Sundgot-Borgen J. Effect of two different weight-loss rates on body composition and strength and power-related performance in elite athletes. Int J Sport Nutr Exerc Metab. 2011;21:97–104.
Elia M, Stubbs RJ, Henry CJ. Differences in fat, carbohydrate, and protein metabolism between lean and obese subjects undergoing total starvation. Obes Res. 1999;7:597–604.
Pasiakos SM, Cao JJ, Margolis LM, Sauter ER, Whigham LD, McClung JP, et al. Effects of high-protein diets on fat-free mass and muscle protein synthesis following weight loss: a randomized controlled trial. FASEB J. 2013;27:3837–47.
Hursel R, Martens EAP, Gonnissen HKJ, Hamer HM, Senden JMG, van Loon LJC, et al. Prolonged adaptation to a low or high protein diet does not modulate basal muscle protein synthesis rates—a substudy. PLoS One. 2015;10:e0137183.
Smith GI, Atherton P, Reeds DN, Mohammed BS, Rankin D, Rennie MJ, et al. Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: a randomized controlled trial. Am J Clin Nutr. 2011;93:402–12.
McGlory C, Wardle SL, Macnaughton LS, Witard OC, Scott F, Dick J, et al. Fish oil supplementation suppresses resistance exercise and feeding-induced increases in anabolic signaling without affecting myofibrillar protein synthesis in young men. Physiol Rep. 2016;4(6). pii:e12715.
Miller BF, Olesen JL, Hansen M, Dossing S, Crameri RM, Welling RJ, et al. Coordinated collagen and muscle protein synthesis in human patella tendon and quadriceps muscle after exercise. J Physiol. 2005;567:1021–33.
Burd NA, West DWD, Moore DR, Atherton PJ, Staples AW, Prior T, et al. Enhanced amino acid sensitivity of myofibrillar protein synthesis persists for up to 24 h after resistance exercise in young men. J Nutr. 2011;141:568–73.
Trommelen J, Holwerda AM, Kouw IWK, Langer H, Halson SL, Rollo I, et al. Resistance exercise augments postprandial overnight muscle protein synthesis rates. Med Sci Sports Exerc. 2016;48:2517–25.
Pennings B, Koopman R, Beelen M, Senden JMG, Saris WHM, van Loon LJC. Exercising before protein intake allows for greater use of dietary protein-derived amino acids for de novo muscle protein synthesis in both young and elderly men. Am J Clin Nutr. 2011;93:322–31.
Atherton PJ, Etheridge T, Watt PW, Wilkinson D, Selby A, Rankin D, et al. Muscle full effect after oral protein: time-dependent concordance and discordance between human muscle protein synthesis and mTORC1 signaling. Am J Clin Nutr. 2010;92:1080–8.
Churchward-Venne TA, Burd NA, Mitchell CJ, West DWD, Philp A, Marcotte GR, et al. Supplementation of a suboptimal protein dose with leucine or essential amino acids: effects on myofibrillar protein synthesis at rest and following resistance exercise in men. J Physiol. 2012;590:2751–65.
Moore DR, Tang JE, Burd NA, Rerecich T, Tarnopolsky MA, Phillips SM. Differential stimulation of myofibrillar and sarcoplasmic protein synthesis with protein ingestion at rest and after resistance exercise. J Physiol. 2009;587:897–904.
Glover EI, Phillips SM, Oates BR, Tang JE, Tarnopolsky MA, Selby A, et al. Immobilization induces anabolic resistance in human myofibrillar protein synthesis with low and high dose amino acid infusion. J Physiol. 2008;586:6049–61.
Devries MC, Breen L, Allmen Von M, Macdonald MJ, Moore DR, Offord EA, et al. Low-load resistance training during step-reduction attenuates declines in muscle mass and strength and enhances anabolic sensitivity in older men. Physiol Rep. 2015;3(8). pii:e12493.
Breen L, Stokes KA, Churchward-Venne TA, Moore DR, Baker SK, Smith K, et al. Two weeks of reduced activity decreases leg lean mass and induces “anabolic resistance” of myofibrillar protein synthesis in healthy elderly. J Clin Endocrinol Metab. 2013;98:2604–12.
Wall BT, Dirks ML, Snijders T, van Dijk J-W, Fritsch M, Verdijk LB, et al. Short-term muscle disuse lowers myofibrillar protein synthesis rates and induces anabolic resistance to protein ingestion. Am J Physiol Endocrinol Metab. 2016;310:E137–47.
Wall BT, Morton JP, van Loon LJC. Strategies to maintain skeletal muscle mass in the injured athlete: nutritional considerations and exercise mimetics. Eur J Sport Sci. 2015;15:53–62.
Tipton KD. Nutritional support for exercise-induced injuries. Sports Med. 2015;45(Suppl 1):S93–104.
Volpi E, Sheffield-Moore M, Rasmussen BB, Wolfe RR. Basal muscle amino acid kinetics and protein synthesis in healthy young and older men. JAMA. 2001;286:1206–12.
Wall BT, Gorissen SH, Pennings B, Koopman R, Groen BBL, Verdijk LB, et al. Aging is accompanied by a blunted muscle protein synthetic response to protein ingestion. PLoS One. 2015;10:e140903–0140913.
Churchward-Venne TA, Holwerda AM, Phillips SM, van Loon LJC. What is the optimal amount of protein to support post-exercise skeletal muscle reconditioning in the older adult? Sports Med. 2016;46:1205–12.
Moore DR, Churchward-Venne TA, Witard O, Breen L, Burd NA, Tipton KD, et al. Protein ingestion to stimulate myofibrillar protein synthesis requires greater relative protein intakes in healthy older versus younger men. J Gerontol A Biol Sci Med Sci. 2015;70:57–62.
Lee SJ, Janssen I, Heymsfield SB, Ross R. Relation between whole-body and regional measures of human skeletal muscle. Am J Clin Nutr. 2004;80:1215–21.
West DWD, Burd NA, Churchward-Venne TA, Camera DM, Mitchell CJ, Baker SK, et al. Sex-based comparisons of myofibrillar protein synthesis after resistance exercise in the fed state. J Appl Physiol. 1985;2012(112):1805–13.
Dreyer HC, Fujita S, Glynn EL, Drummond MJ, Volpi E, Rasmussen BB. Resistance exercise increases leg muscle protein synthesis and mTOR signalling independent of sex. Acta Physiol (Oxf). 2010;199:71–81.
Smith GI, Reeds DN, Hall AM, Chambers KT, Finck BN, Mittendorfer B. Sexually dimorphic effect of aging on skeletal muscle protein synthesis. Biol Sex Differ. 2012;3:11.
Isidori AM, Giannetta E, Greco EA, Gianfrilli D, Bonifacio V, Isidori A, et al. Effects of testosterone on body composition, bone metabolism and serum lipid profile in middle-aged men: a meta-analysis. Clin Endocrinol (Oxf). 2005;63:280–93.
Smith GI, Atherton P, Villareal DT, Frimel TN, Rankin D, Rennie MJ, et al. Differences in muscle protein synthesis and anabolic signaling in the postabsorptive state and in response to food in 65–80 year old men and women. PLoS One. 2008;3:e1875.
Guillet C, Delcourt I, Rance M, Giraudet C, Walrand S, Bedu M, et al. Changes in basal and insulin and amino acid response of whole body and skeletal muscle proteins in obese men. J Clin Endocrinol Metab. 2009;94:3044–50.
Murton AJ, Marimuthu K, Mallinson JE, Selby AL, Smith K, Rennie MJ, et al. Obesity appears to be associated with altered muscle protein synthetic and breakdown responses to increased nutrient delivery in older men, but not reduced muscle mass or contractile function. Diabetes. 2015;64:3160–71.
Tran L, Kras KA, Hoffman N, Ravichandran J, Dickinson JM, D’Lugos A, et al. Lower fasted-state but greater increase in muscle protein synthesis in response to elevated plasma amino acids in obesity. Obesity (Silver Spring). 2018;26:1179–87.
Smeuninx B, Mckendry J, Wilson D, Martin U, Breen L. Age-related anabolic resistance of myofibrillar protein synthesis is exacerbated in obese inactive individuals. J Clin Endocrinol Metab. 2017;102:3535–45.
Biolo G, Tipton KD, Klein S, Wolfe RR. An abundant supply of amino acids enhances the metabolic effect of exercise on muscle protein. Am J Physiol. 1997;273:E122–9.
Masiero E, Agatea L, Mammucari C, Blaauw B, Loro E, Komatsu M, et al. Autophagy is required to maintain muscle mass. Cell Metab. 2009;10:507–15.
Castets P, Lin S, Rion N, Di Fulvio S, Romanino K, Guridi M, et al. Sustained activation of mTORC1 in skeletal muscle inhibits constitutive and starvation-induced autophagy and causes a severe, late-onset myopathy. Cell Metab. 2013;17:731–44.
Kitajima Y, Tashiro Y, Suzuki N, Warita H, Kato M, Tateyama M, et al. Proteasome dysfunction induces muscle growth defects and protein aggregation. J Cell Sci. 2014;127:5204–17.
Bell RAV, Al-Khalaf M, Megeney LA. The beneficial role of proteolysis in skeletal muscle growth and stress adaptation. Skelet Muscle. 2016;6:16.
Wagenmakers AJ. Tracers to investigate protein and amino acid metabolism in human subjects. Proc Nutr Soc. 1999;58:987–1000.
Burd NA, Hamer HM, Pennings B, Pellikaan WF, Senden JMG, Gijsen AP, et al. Substantial differences between organ and muscle specific tracer incorporation rates in a lactating dairy cow. PLoS One. 2013;8:e68109.
Smeets JSJ, Horstman AMH, Schijns OEMG, Dings JTA, Hoogland G, Gijsen AP, et al. Brain tissue plasticity: protein synthesis rates of the human brain. Brain. 2018;141:1122–9.
Nair KS, Halliday D, Griggs RC. Leucine incorporation into mixed skeletal muscle protein in humans. Am J Physiol. 1988;254:E208–13.
Holwerda AM, Kouw IWK, Trommelen J, Halson SL, Wodzig WK, Verdijk LB, et al. Physical activity performed in the evening increases the overnight muscle protein synthetic response to presleep protein ingestion in older men. J Nutr. 2016;146:1307–14.
Nair KS, Ford GC, Ekberg K, Fernqvist-Forbes E, Wahren J. Protein dynamics in whole body and in splanchnic and leg tissues in type I diabetic patients. J Clin Investig. 1995;95:2926–37.
Adey D, Kumar R, McCarthy JT, Nair KS. Reduced synthesis of muscle proteins in chronic renal failure. Am J Physiol Endocrinol Metab. 2000;278:E219–25.
Kim I-Y, Shin Y-A, Schutzler SE, Azhar G, Wolfe RR, Ferrando AA. Quality of meal protein determines anabolic response in older adults. Clin Nutr. 2017;37:2076–83.
Kim I-Y, Schutzler S, Schrader A, Spencer H, Kortebein P, Deutz NEP, et al. Quantity of dietary protein intake, but not pattern of intake, affects net protein balance primarily through differences in protein synthesis in older adults. Am J Physiol Endocrinol Metab. 2015;308:E21–8.
Pennings B, Pellikaan WF, Senden JMG, van Vuuren AM, Sikkema J, van Loon LJC. The production of intrinsically labeled milk and meat protein is feasible and provides functional tools for human nutrition research. J Dairy Sci. 2011;94:4366–73.
Elango R, Ball RO, Pencharz PB. Recent advances in determining protein and amino acid requirements in humans. Br J Nutr. 2012;108(Suppl 2):S22–30.
Mazzulla M, Volterman KA, Packer JE, Wooding DJ, Brooks JC, Kato H, et al. Whole-body net protein balance plateaus in response to increasing protein intakes during post-exercise recovery in adults and adolescents. Nutr Metab. 2018;15:62.
Mitchell CJ, Churchward-Venne TA, Parise G, Bellamy L, Baker SK, Smith K, et al. Acute post-exercise myofibrillar protein synthesis is not correlated with resistance training-induced muscle hypertrophy in young men. PLoS One. 2014;9:e89431.
Damas F, Phillips SM, Libardi CA, Vechin FC, Lixandrao ME, Jannig PR, et al. Resistance training-induced changes in integrated myofibrillar protein synthesis are related to hypertrophy only after attenuation of muscle damage. J Physiol. 2016;594:5209–22.
Brook MS, Wilkinson DJ, Mitchell WK, Lund JN, Szewczyk NJ, Greenhaff PL, et al. Skeletal muscle hypertrophy adaptations predominate in the early stages of resistance exercise training, matching deuterium oxide-derived measures of muscle protein synthesis and mechanistic target of rapamycin complex 1 signaling. FASEB J. 2015;29:4485–96.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No sources of funding were used to assist in the preparation of this article.
Conflict of interest
Jorn Trommelen and Luc van Loon have received research grants, consulting fees, speaking honoraria, or a combination of these, from Friesland Campina and PepsiCo. Milan Betz has no potential conflicts of interest relevant to the content of this review.
Rights and permissions
OpenAccess This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Trommelen, J., Betz, M.W. & van Loon, L.J.C. The Muscle Protein Synthetic Response to Meal Ingestion Following Resistance-Type Exercise. Sports Med 49, 185–197 (2019). https://doi.org/10.1007/s40279-019-01053-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-019-01053-5